Anatomy In Surgery: Learning And Teaching Through Drawings
By Emmanuel P. Estrella, MD, MSc
As a hand surgeon, I am involved in a university-based hospital–University of the Philippines-Philippine General Hospital–where encounters with medical students and orthopedic surgery residents is a daily routine. We try to create an atmosphere in the operating room where learning is for everyone, both surgeons and students alike.
As surgeons, we always prepare for a surgery no matter how simple or complex it may be. Preparation starts with familiarizing ourselves with the human anatomy. In cases that I do not do that often or in cases of complex reconstruction, I always do a “pre-operative” sketch of a surgical plan, which I bring to the operating room with me as a reference. Here we can discuss with the residents our “battle plan.”
On the day of the surgery, I carry along a pilot’s luggage with all my necessary stuff for a medium or major case (Figure 1). This would include my surgical loupes, surgical instruments, nerve stimulator, several Coban bandages, the not so common nylon 11-0 sutures, and of course, a small bluetooth speaker. My surgery is never complete without my 70’s and 80’s playlist. Such music choice has become my trademark, which my anesthesiologist and surgical staff have looked forward to. Somehow, music keeps me and the surgical staff relaxed despite a lengthy and difficult surgery.

Figure 1
After my surgery, I again hit my drawing pad to sketch out my operative findings, noting as well all the steps, difficulties encountered, and lessons learned from the operation. This is a practice that I started doing at the start of my fellowship in microsurgery under Professor Kazuteru Doi, in Japan (2002), and subsequently with Dr. PC Ho in Hong Kong (2004). Dr. PC Ho’s post-operative drawings made it easier to understand what went on during the surgery. I usually try to draw the key steps of a surgical procedure right after the surgery in order to familiarize myself with the procedure since an intraoperative picture usually helps me remember. Aside from the drawings, I always include some “Pearls & Pitfalls” of that particular surgery: what went wrong, what techniques made surgery easier, and why surgery was too long, among others. In so doing, I avoid committing the same mistakes from the same procedure in the future. One of the cases we do now with increasing frequency is free muscle transfer for elbow flexion in brachial plexus injuries. This drawing, which was done way back in 2010, helped me in subsequent cases and eventually shortened our operative time during surgery (Figure 2). This case always helped me remember how to look for the thoraco-acromial artery, manage vessel diameter mismatch, and watch out for the transverse cervical arteries during spinal accessory nerve dissection. In Figure 3, a replantation procedure was managed with vein grafts for both artery and venous anastomosis. The decision to use a Y-graft was based on the prolonged ischemia time of the amputated part, which worked well during the replantation surgery.
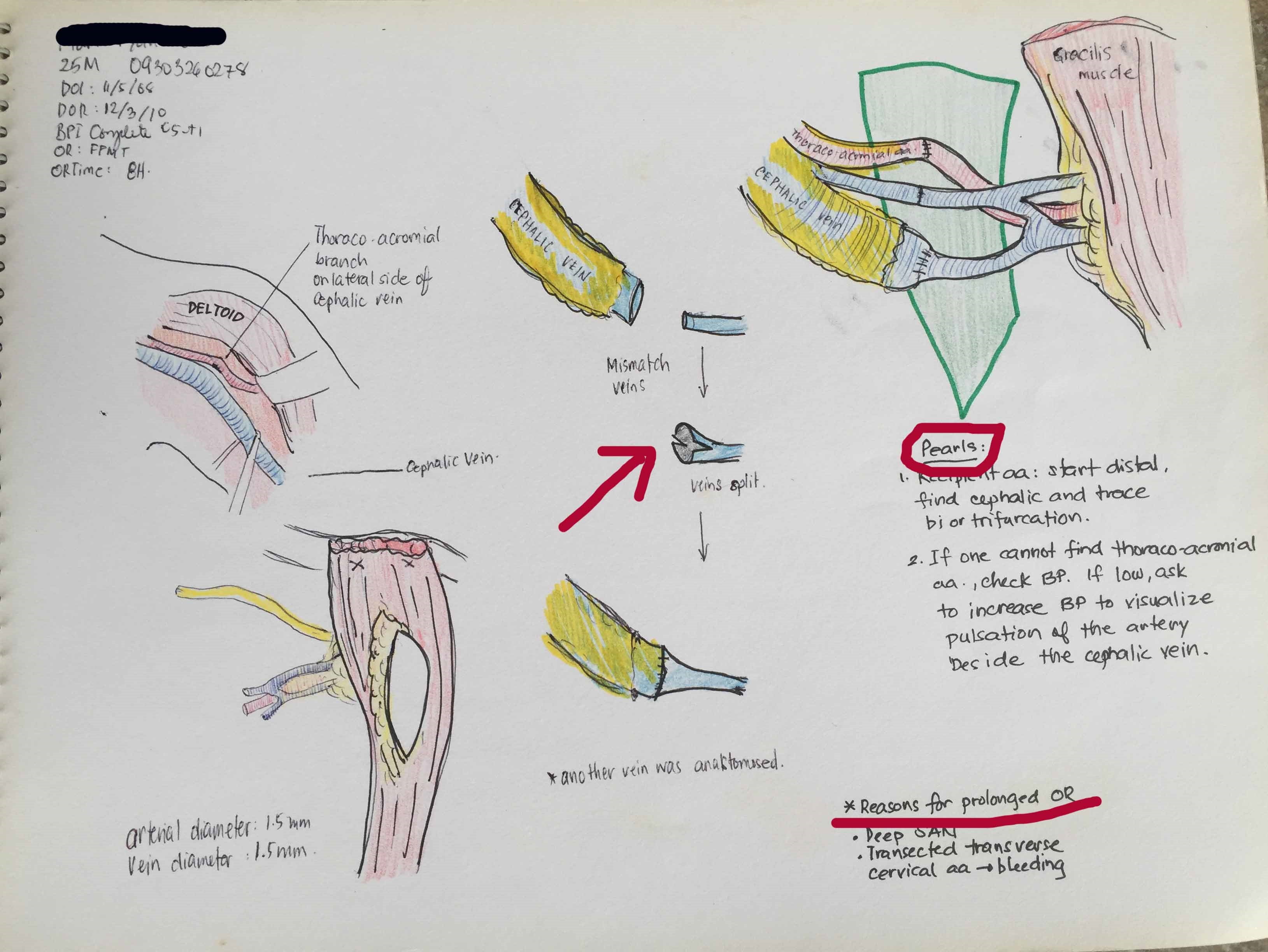
Figure 2
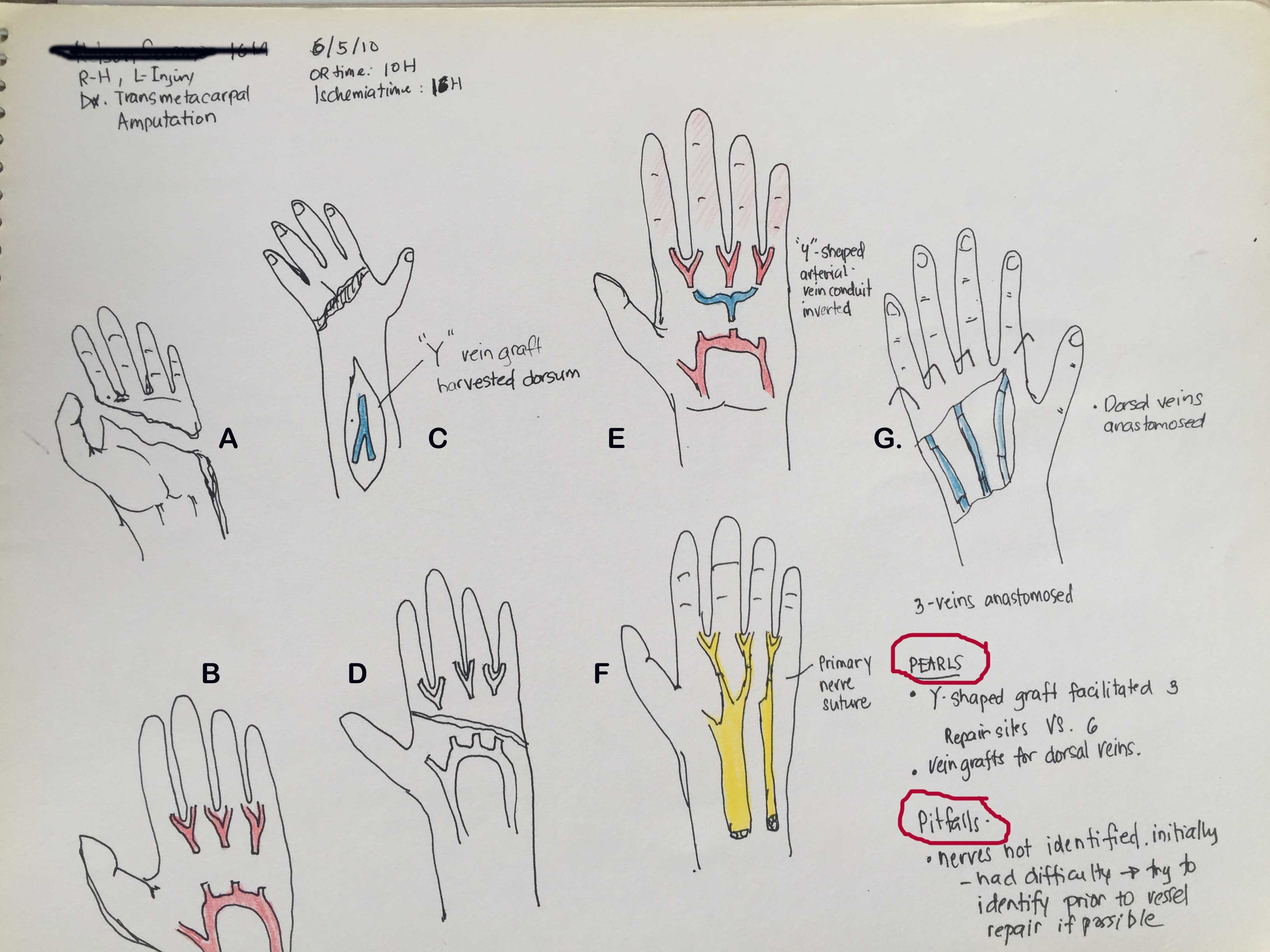
Figure 3
Through the years, I’ve accumulated a number of sketchpads on my surgeries (Figure 4), cases that I consider interesting, challenging or difficult. Even though we do some cases routinely, we still learn a few things from every surgical procedure. I believe that one way of familiarizing one’s self with the anatomy is by being able to draw it. I try to teach this to our orthopedic residents and rotating medical students. This way, it makes it easier to understand fracture patterns and fixations, operative findings or reconstructions.
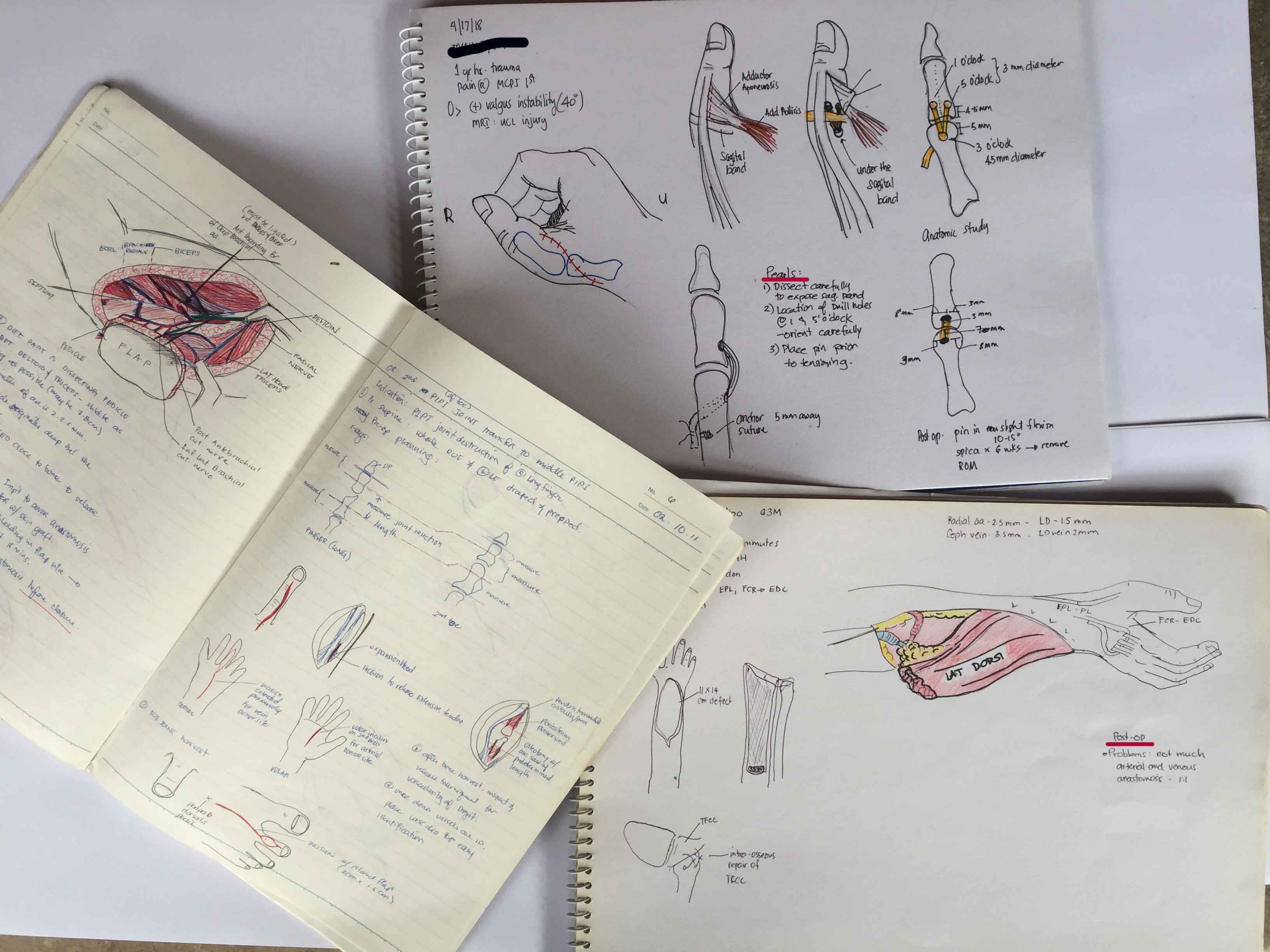
Figure 4
Reference:
Stewart S, Charon R. Art, Anatomy, Learning, and Living. JAMA. 2002;287(9):1182. doi:10.1001/jama.287.9.1182-JMS0306-5-1