My Approach for This Chronic Lunate Dislocation
By Chris LaSalle, MD


The patient is a 45-year-old male who was unfortunately involved in a motor vehicle accident in Tennessee. His injury occurred on June 16, 2018. He was seen there and transferred to home, seen by my physician assistant on July 5, 2018, and found to have a lunate dislocation. I saw him early the next week and planned for surgical intervention. The technique described below uses a 2.7 mm cannulated drill and the Arthrex tight-rope. I harvest about 1/3 of the flexor carpi radialis for my graft, leaving it attached to the index metacarpal. I have been using this technique for my chronic scapholunate (SL) injuries. Several patients have at least 1 year follow-up, including this case. In my SL injuries, I have seen the SL interval widen, but have kept the scaphoid out of flexion and the lunate out of extension. The cost is the price of the Arthrex tight rope and whatever anchors to fixate the graft on the dorsum of the wrist. I am in private practice and have no access to a lab. Below is the operative note:
DESCRIPTION OF PROCEDURE:
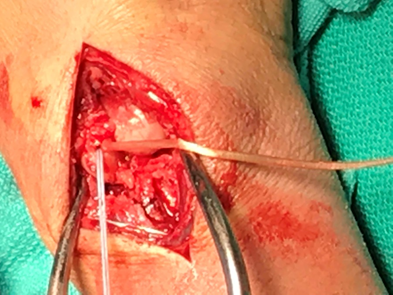
After adequate regional anesthetic was obtained, the right arm was prepared and draped in sterile fashion. Tourniquet inflated to 250 mmHg. I began with a longitudinal incision central over the wrist centering over the middle metacarpal and over the Lister’s tubercle. Blunt dissection through subcutaneous tissue. Bleeding points were halted with electrocautery. The extensor pollicis longus was identified and the 3rd dorsal compartment opened up and the extensor pollicis longus (EPL) retracted radialward. I then sharply elevated up the wrist capsule off the distal radius. I was careful to preserve the 4th dorsal compartment tendons, as well as the 2nd dorsal compartment tendons. There was a small osteophyte of bone that was removed from a previous avulsion. I did see this on x-ray. I then exposed the dorsal aspect of the wrist joint. The scaphoid was reduced as was the triquetrum. However, the lunate was volarly dislocated. With traction and a moderate amount of difficulty, I was able to remove the hematoma and all the soft tissue and reduce the lunate.
This was highly unstable. His lunotriquetral (LT) and scapholunate (SL) ligaments were essentially gone. I saw nothing to repair. At that point, I decided to do a scapholunate and LT ligament reconstruction. I then went volarward. A longitudinal incision was made at the radial border of the 4th digit, starting at the superficial palmar arch. This was taken across the wrist taken transversely radially and then longitudinally up into the wrist joint itself. Skin flaps were elevated. I bluntly dissected and exposed the median nerve. This was unroofed from proximal to distal. The median nerve itself looked quite good. I completely exposed the carpal canal. I then exposed the volar aspect of the wrist. There was a classic transverse ligament laceration as the ligaments had been avulsed directly off the radius. I put a 3-0 Ethibond stitch in the volar capsule to try and tighten this up. I really did not have much in the way to sew to because again, this had been avulsed off the distal radius. I then exposed the flexor carpi radialis. I carefully mobilized this and identified the tip of the scaphoid volarward.
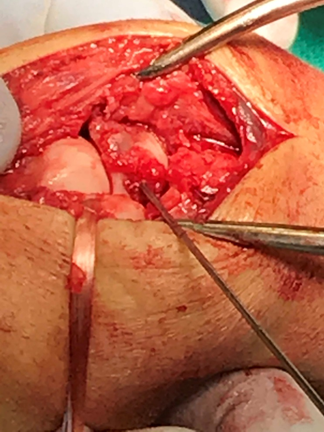
My attention was then turned dorsally. I placed a K-wire starting at the dorsal ulnar aspect of the scaphoid at the scapholunate joint. I then carefully advanced this under image intensification. I had to make a couple of adjustments to get this in the exact position that I wanted, but I made sure that pin and the guidewire exited at the tip of the scaphoid. I was very pleased with my overall placement. Again, my placement was slightly dorsal and at the joint surface between the scaphoid and lunate.


I then used a 2.7 mm cannulated drill and created a hole in the scaphoid. I identified this volarward. I was careful to remove bony fragments while I drilled to prevent any burning of the bone.

I then made a transverse incision in the mid forearm region, identified the flexor carpi radialis (FCR). I carefully mobilized this from its subcutaneous tissue. This ulnar portion of the FCR of about little over 25-30 of the tendon was transected proximally and pulled up distalward. This turned out to be a little under a one-third of the FCR tendon. I used a Hewson suture passer and then passed this through the scaphoid and placed a whipstitch with 3-0 Ethibond in the free edge of the flexor carpi radialis. I then shuttled this up through the scaphoid along with an Arthrex TightRope. The button went beautifully right up against the scaphoid tubercle and the tendon graft went nicely through the scaphoid itself.
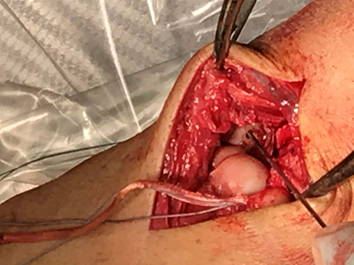
I then turned my attention back dorsally again. The lunate had redislocated as I was working with the scaphoid. I brought this back up again. With a guidewire from the Arthrex set, I was trying to pass the guidewire through the central portion of the lunate and through the central portion of the triquetrum. Each time I attempted I was too volar on the lunate exiting ulnarward. I could not drop my hand enough to adequately get this directly across and the triquetrum tended to fall into a dorsal-type position and I had a hard time holding this down. I elected to place just the hole in through the lunate.
I then drilled this with a 2.7 mm cannulated drill. After I had created my tunnel in the lunate, I allowed the lunate to volarly dislocate again, giving me excellent exposure to the triquetrum, and then drilled a guide pin through the triquetrum confirming both of these under image intensification.

I then used my 2.7 mm drill to create a hole through the triquetrum. The guide pin poked ulnarward and into the hand and I made a stab incision ulnarward and then bluntly dissected down to identify the guide pin.

Instrumentation was then removed. I had a difficult time getting the holes to line up perfectly between the lunate and the triquetrum. Using the blunt tipped pin from the TightRope set, I was able to pass this through the lunate and with a moderate amount of difficulty, pass this through the triquetrum and then carefully out the ulnar side of the hand. I identified this ulnarward.

This had the loop on the scaphoid side and I placed the 3-0 Ethibond core stitch and the TightRope through this and shuttled this through the lunate, through the triquetrum, and out the ulnar side of the hand. This passed my graft beautifully through the lunate and the triquetrum.

With the TightRope, I was able to tension this and beautifully keep the lunate reduced as well as close down the scapholunate interval. This also gave me wonderful stability between the lunate and the triquetrum.
I then passed the tendon graft over the dorsum of the wrist for later reattachment to the scaphoid itself. I then trimmed the TightRope and placed the button ulnarward. I placed a single throw and tightened this down. I had a great reduction. This was confirmed under image intensification. The button was not quite all the way down up against the triquetrum.

I held this in place and then placed a 0.045 K-wire through the scaphoid into the capitate and then 1 into the scaphoid and into the lunate for provisional fixation to hold my reduction.

I then vigorously pulled on the FiberWire sutures to make sure that I did not violate my trough or cut my graft. I then pulled on my graft. This also had excellent stability, so I did not disrupt these with the K-wires. I then tied the button ulnarward. I got this as close to the triquetrum as possible with only about a millimeter away from the bone itself. I was extremely pleased at how well this moved as well as how well this held the proximal carpal row in good stability. This was then trimmed off. Prior to tensioning this and prior to putting the K-wires in, I irrigated the volar aspect of the wrist and closed this with 5-0 and 4-0 nylon sutures. I then again tied the button ulnarward and passed my K-wires prior to tightening this button. I then passed the tendon graft through the ulnar limb of the capsule and the radial limb of the capsule, functionally using the tendon graft to help me close the dorsal wrist capsule. This also tensioned my graft quite nicely and gave me something excellent to sew to. I was a little hesitant to place an anchor in the scaphoid or the lunate for fear of disrupting my tunnels that I had already drilled through these bones. I sutured this in place along with a capsular repair of multiple 3-0 Ethibond sutures. Prior to this, I did irrigate copious amounts of normal saline. The subcutaneous tissue closed with 3-0 Vicryl, skin reapproximated with 4-0 nylon and 4-0 nylon was used to close the ulnar-sided wound. The K-wires were bent over and cut short. He was placed in a well-molded thumb spica splint and the tourniquet was deflated at 2 hours, and he was transferred to the recovery room without difficulty.

These are radiographs at one year post-op. He has developed significant scaphocapitate degenerative changes and still has some pain. He has 50 degrees of extension and 60 degrees of flexion. When I preform this surgery for a SL disruption I will pin and drill the lunate and triquetrum at the same time. One pearl is to get as low as possible on the lunate and keep my hand low. Otherwise I will get too volar on the triquetrum. If anyone has any comments or questions please email me at **Please contact ASSH Staff member Kendall for this information, ksteinle@assh.org.**